 |
Close
window to return
|
Issue 3, January 1999, pp.12-13.
How does relative
deprivation affect health?
Malcolm MacLeod, Elspeth Graham, Marie Johnston, Chris Dibben and
Irene Morgan
Introduction
There is now compelling evidence that poor health is not simply the outcome
of poverty and absolute deprivation. If it were, then those in the poorest
circumstances would have the poorest health, while everyone above the
poverty line would enjoy the same level of good health. Instead there
is a graded relationship between income or socio-economic status and health,
with relative improvements in income and living standards associated with
relative improvements in levels of health. Further, societies in which
there are wide inequalities in income and living standards have lower
life expectancies than societies in which income differences are smaller.
In the UK, both income differences and health inequalities have increased
over the last few decades despite substantial rises in standards of living.
This has led Wilkinson(1) to conclude that health is related to social
relativities rather than absolute standards of living. This finding, if
substantiated by detailed studies, has important implications for public
policy where initiatives and resources are often targeted on particular
areas defined as deprived. If health status is dependent on relative rather
than absolute living standards, the effects of such policies may be limited
because of their failure to take into account income disparities across
society as a whole. Improving conditions for the poorest could have little
or no impact if their position relative to other groups remains static
or worsens.
Social Geography
Recent research has shown that the relationship between relative deprivation
and health, apparent at the national scale, also exists at sub-national
levels within the UK and that it can be related to local social geography.
Gatrell,(2) for example, used spatial data (census wards) for one health
authority in north-west England to demonstrate that a measure of relative
deprivation which takes account of the location of areas in relation to
each other performs well as a correlate of both all-cause mortality and
mortality due to ischaemic heart disease. We have been able to demonstrate
a similar relationship for our study area in Scotland using age-standardised
self-reported limiting long-term illness from the 1991 census as our measure
of health. However, we have also found that the direction of the relationship
between relative spatial deprivation and health is reversed when the deprivation
scores for the wards themselves are added to the model. This is best explained
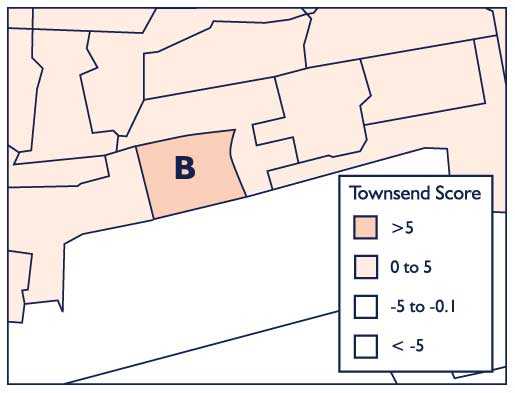
by reference to Figure 1 which illustrates the detailed patterns of deprivation
in two different parts of the City of Dundee.
Figure 1: Varying patterns of deprivation in the City of Dundee
In the city as a whole, we found that deprivation scores for small areas
(census output areas) are positively associated with levels of limiting
long-term illness in these areas. Standardising for this relationship,
we then investigated the relationship between deprivation levels in surrounding
areas and levels of limiting long-term illness in given census areas.
Preliminary results, which show a modest but significant relationship,
are intriguing. They suggest that an area, such as area A in Figure 1,
which has a lower level of deprivation than its nearest neighbours records
higher levels of limiting long-term illness than might be expected from
its own deprivation score alone. The opposite is true of areas, like area
B, which are surrounded by less deprived neighbours. Such areas exhibit
lower levels of ill-health than we are led to expect by solely considering
their own levels of deprivation. Thus it seems that highly local social
relativities are influencing health but in the opposite way to that suggested
by other research conducted at larger spatial scales. In health terms,
being surrounded by less deprived neighbours appears to confer an advantage,
whereas having neighbouring areas with higher levels of deprivation seems
to 'pull down' an area and result in greater ill health relative to other
areas with the same level of (internal) deprivation. These findings are
still preliminary but they raise a further question, 'What kind of mechanism
could explain the relationship between spatial aspects of deprivation
and health?'
Social Comparisons
Given that, at an individual level, what may be most important with regards
to relative deprivation is whether one perceives oneself to be disadvantaged
relative to other people, it would seem reasonable to suppose that psychological
factors are in some way involved. We already know that psychological factors
(e.g. depression) can affect health and that such factors are also associated
with health-related behaviours (e.g. diet and exercise) which, in turn,
are related to health. The principal question then becomes, 'Is there
any mechanism that could make a plausible link between spatial aspects
of deprivation and those psychological factors known to be related to
health?'
The fact that contrasting social geographies seem to be related to health
differentials suggests that the relative comparisons made by people living
in neighbouring areas may be a vital component in explaining inequalities
in health. Thus there may be a role for social comparisons in explaining
the relationship between relative deprivation and health (see Figure 2).
Figure 2: Schematic representation of possible relationship between
relative deprivation and health
We often engage in making social comparisons with others as a way of evaluating
ourselves. The social comparisons we make have many facets but one that
may prove particularly important is the direction of the comparison. Many
psychological studies have indicated that making downward comparisons
(i.e. with people who are worse off than you in some respect) can bolster
or enhance one's self-esteem and generally tends to be associated with
more positive outcomes than if we make upward comparisons (i.e. with people
who are better off). In addition, there may be a life course dimension
in the social comparisons we make in that the extent to which one believes
one is relatively deprived may be influenced by prior life experiences
(e.g. number of episodes of poverty) and/or the perception of changing
levels of material affluence in society.
Our Study
Our study is currently examining the issue of how the social comparisons
we make might influence recovery from illness. Does comparing oneself
with people who are worse-off in economic terms facilitate recovery? In
order to address such questions, our study has married the varied skills
and expertise of health and social geographers with those of health and
social psychologists. Specifically, we are following the pattern of recovery
in 200 patients in the city of Dundee and surrounding areas who have suffered
a first myocardial infarction (MI). Patients are being recruited from
the Cardiac Rehabilitation Unit of Ninewells Hospital in Dundee over a
2-year period. Our data (collected via face-to-face interviews with patients)
will allow us to construct a range of spatial and economic indices and
provide measures of health outcome and of potential mediating variables
such as depression, self-esteem and health-related behaviours. In particular,
we will be concerned with the extent to which social comparison processes
made at 5-6 weeks post-MI are predictive of recovery three months later.
We hope to be able to: determine how important comparison processes are
for explaining the relationship between relative deprivation and health;
examine whether social deprivation factors operate via psychological factors
(including beliefs and emotional states) and health behaviours already
shown to be linked to health outcomes; establish those indices of social
inequality which are most clearly related to health; and determine the
psychological and spatial conditions that are most likely to give rise
to perceived relative deprivation.
Policy Implications
Through an increased understanding of such relationships, it may prove
possible in the future to develop policies and interventions that will
ultimately lead to improvements in the health and well-being of the general
population. In particular, if we find that social comparisons are an important
explanatory mechanism in the relationship between relative deprivation
and health, then local and national health care strategies concerned with
recovery from MI may find this research valuable in the effective targeting
of resources, and the education of health care professionals.
Malcolm MacLeod, Elspeth Graham and Chris Dibben are based in the School
of Geography.
Marie Johnston and Irene Morgan are based in the School of Psychology
at the University of St Andrews.
References:
1. Wilkinson, R. G. (1996) Unhealthy Societies, London : Routledge.
2. Gatrell, A. (1998) 'Structures of geographical and social space and
their consequences for human health' Geografiska Annaler, 79 (3)
pp.141-154.